Tag: opioid
-

BCBS Alabama to No Longer Cover OxyContin Beginning in 2019
BIRMINGHAM, AL – Effective Jan. 1, 2019, Blue Cross Blue Shield of Alabama will no longer cover OxyContin for members with the exception of Blue Advantage members. This is in response to concerns for members’ care and safety. Since 2015, opioid prescriptions in the U.S. and in Alabama have declined. Over the last two years,…
-

Overshadowed by Opioids, Meth is Back and Hospitalizations Surge
The number of people hospitalized because of amphetamine use is skyrocketing in the United States, but the resurgence of the drug largely has been overshadowed by the nation’s intense focus on opioids. Amphetamine-related hospitalizations jumped by about 245 percent from 2008 to 2015, according to a recent study in the Journal of the American Medical Association. That…
-

Alabama Medicaid Alert: Short-Acting Opioid Naïve Limits
Effective Nov: 1, 2018, the Alabama Medicaid Agency will begin implementing limits on short-acting opiates for opioid naïve recipients. The Agency defines “opioid naïve” as a recipient with no opioid claim in the past 180 days. Edit Details: A 7-day supply limit for adults age 19 and older A 5-day supply limit for children age 18…
-

POLL: Rural Americans “Profoundly Worried” about Opioid Crisis
BOSTON — According to a new NPR/Robert Wood Johnson Foundation/Harvard T.H. Chan School of Public Health poll, rural Americans cite drug/opioid abuse as the biggest problem facing their local community (25 percent), followed by economic concerns (21 percent). The poll of 1,300 adults living in the rural United States found that a majority of rural Americans…
-

Congress Passes New Opioid Package; Awaiting Presidential Signature
Earlier this week Congress reached agreement on legislation to address the opioid epidemic with the passage of the “SUPPORT for Patients and Communities Act,” which President Donald Trump is expected to sign. The legislation touches on almost every aspect of the epidemic and includes numerous provisions to expand access to substance-use disorder (SUD) prevention and treatment…
-
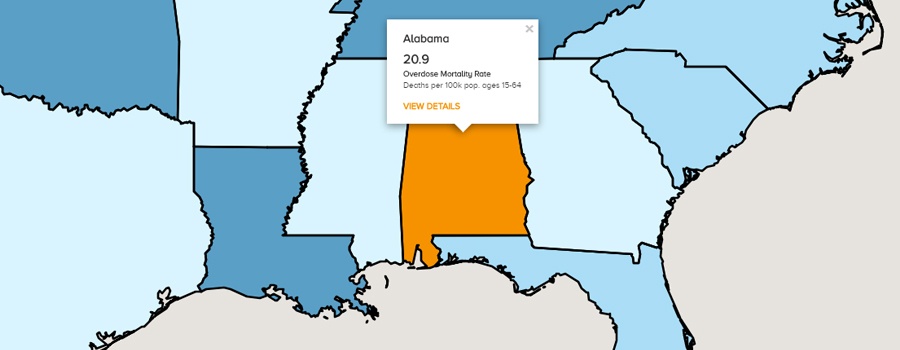
New Interactive Map Shows How Alabama Measures Up in the National Opioid Crisis
WASHINGTON, Oct. 4, 2018 – A new interactive data tool launched by the United States Department of Agriculture and NORC at the University of Chicago shows for the first time an in-depth, county-by-county, look at the impact of the opioid epidemic across the entire country. The tool is intended to help leaders build grassroots strategies to…
-

Alabama Medicaid Agency Updates
Short-Acting Opioid Naïve Limits — Effective Nov. 1 Effective Nov. 1, 2018, the Alabama Medicaid Agency will begin implementing limits on short-acting opiates for opioid naïve recipients. The Agency defines “opioid naïve” as a recipient with no opioid claim in the past 180 days. Edit Details: A 7-day supply limit for adults age 19 and older…
-

ProAssurance and Sure Med Compliance Join to Fight Opioid Crisis
BIRMINGHAM ─ ProAssurance Corporation has announced an exclusive affiliation with Sure Med Compliance® (SMC) to promote the use of SMC’s Care Continuity Program® (CCP) in an effort to help combat the opioid epidemic in the United States. ProAssurance-insured physicians will be eligible for discounted access to Sure Med’s Care Continuity Program The CCP helps physicians…
-

Reducing Opioid Prescriptions for One Operation Can Have a Spillover Effect to Other Procedures
Study results show revised recommendations resulted in about 17 fewer pills being dispensed per patient for four major operations. CHICAGO – To curb the use of opioids after major elective operations and prevent these pain relievers from falling into the wrong hands, surgeons at the University of Michigan developed prescribing recommendations based on published medical…
-